Associations among High-Quality Protein and Energy Intake, Serum Transthyretin, Serum Amino Acids and Linear Growth of Children in Ethiopia

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Study Population
2.2. Data Collection
2.3. Dietary Assessment
2.4. Anthropometrics Assessment
2.5. Biochemical Assessment
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
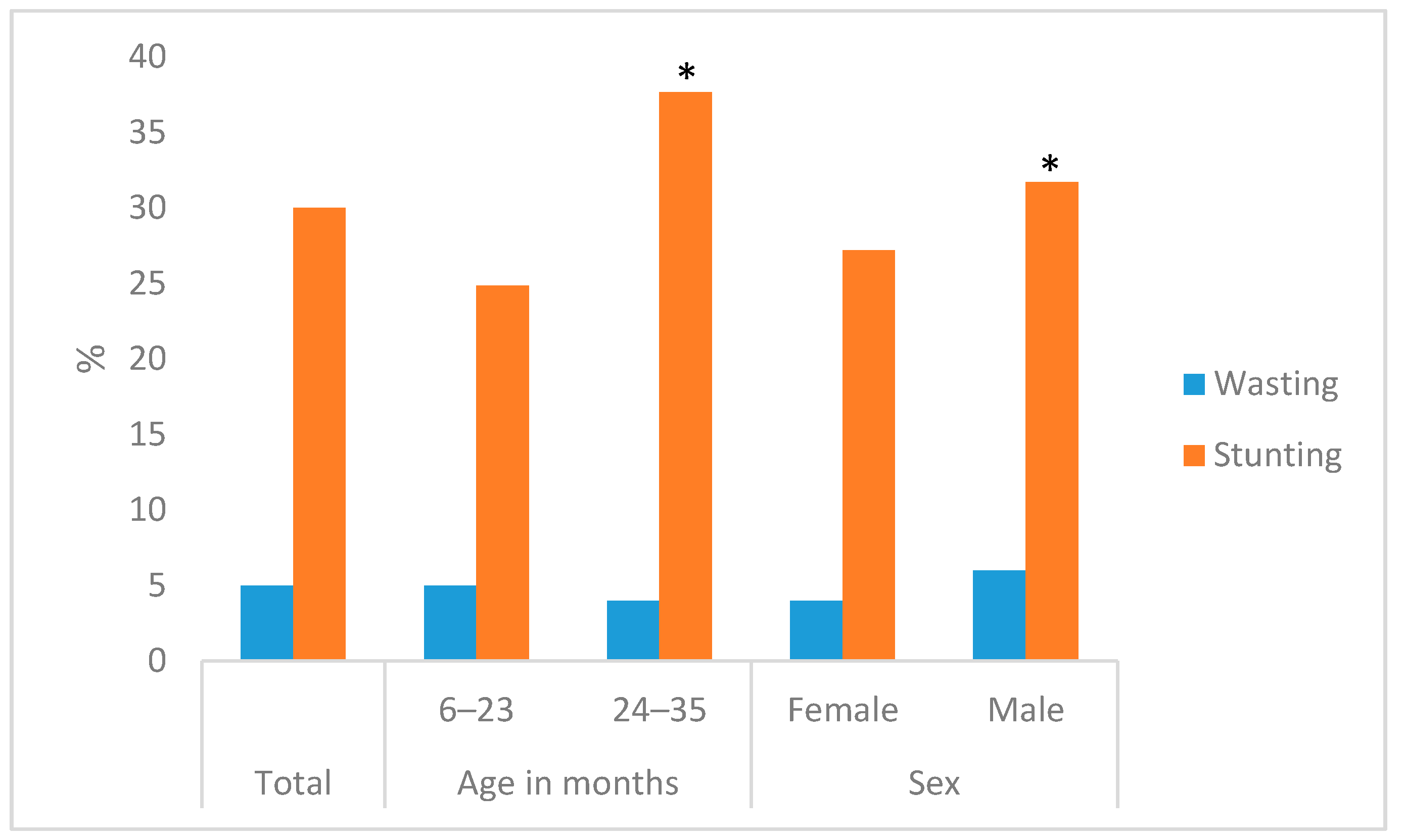
3.2. Feeding Indicators and Child Characteristics
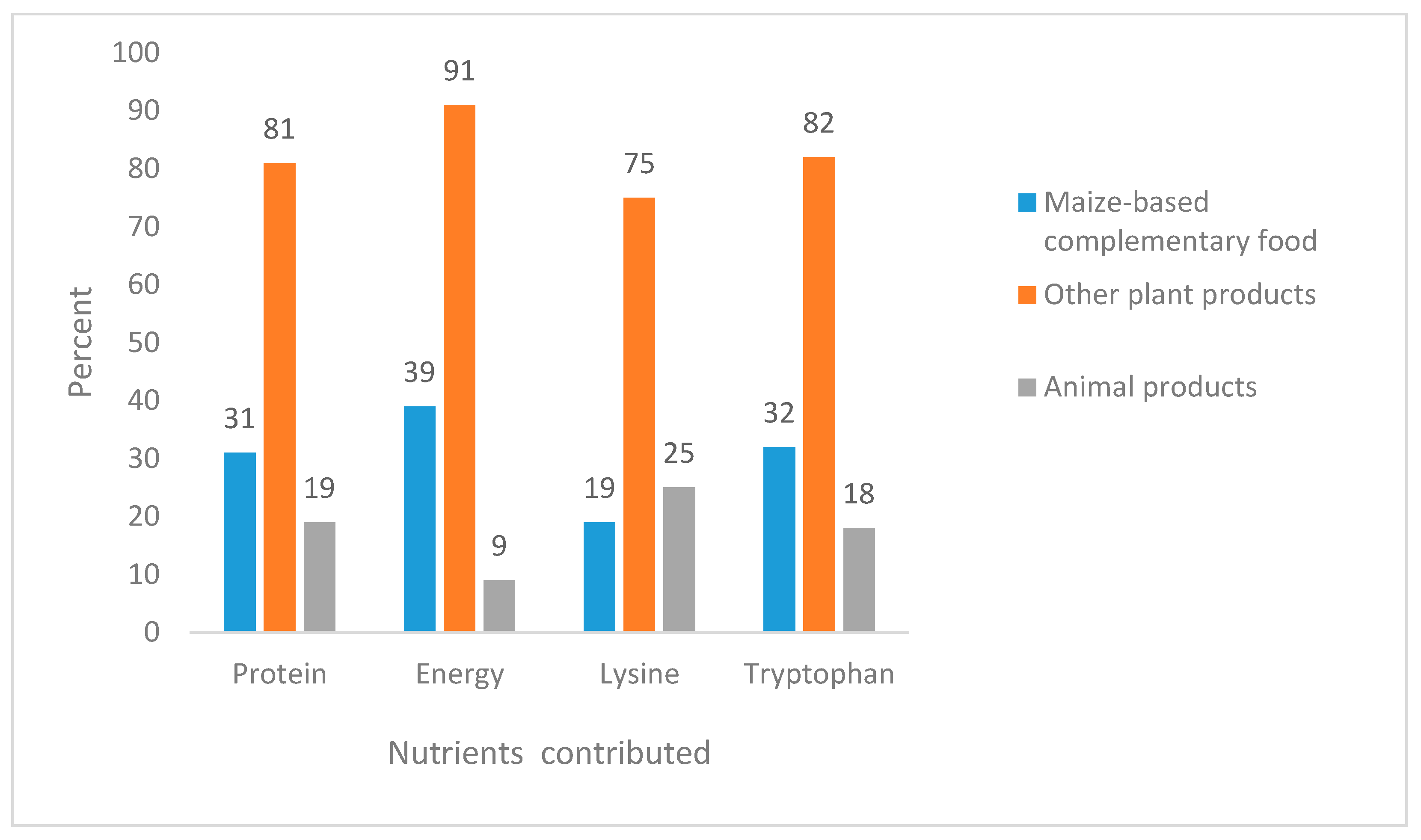
3.3. Dietary High-Quality Protein and Energy Intake of Children
3.4. Protein Biomarkers of Children
3.5. Correlations among Intake of Essential Amino Acids, Serum Transthyretin, Serum Amino Acids, Serum IGF-1 and Children’s Growth
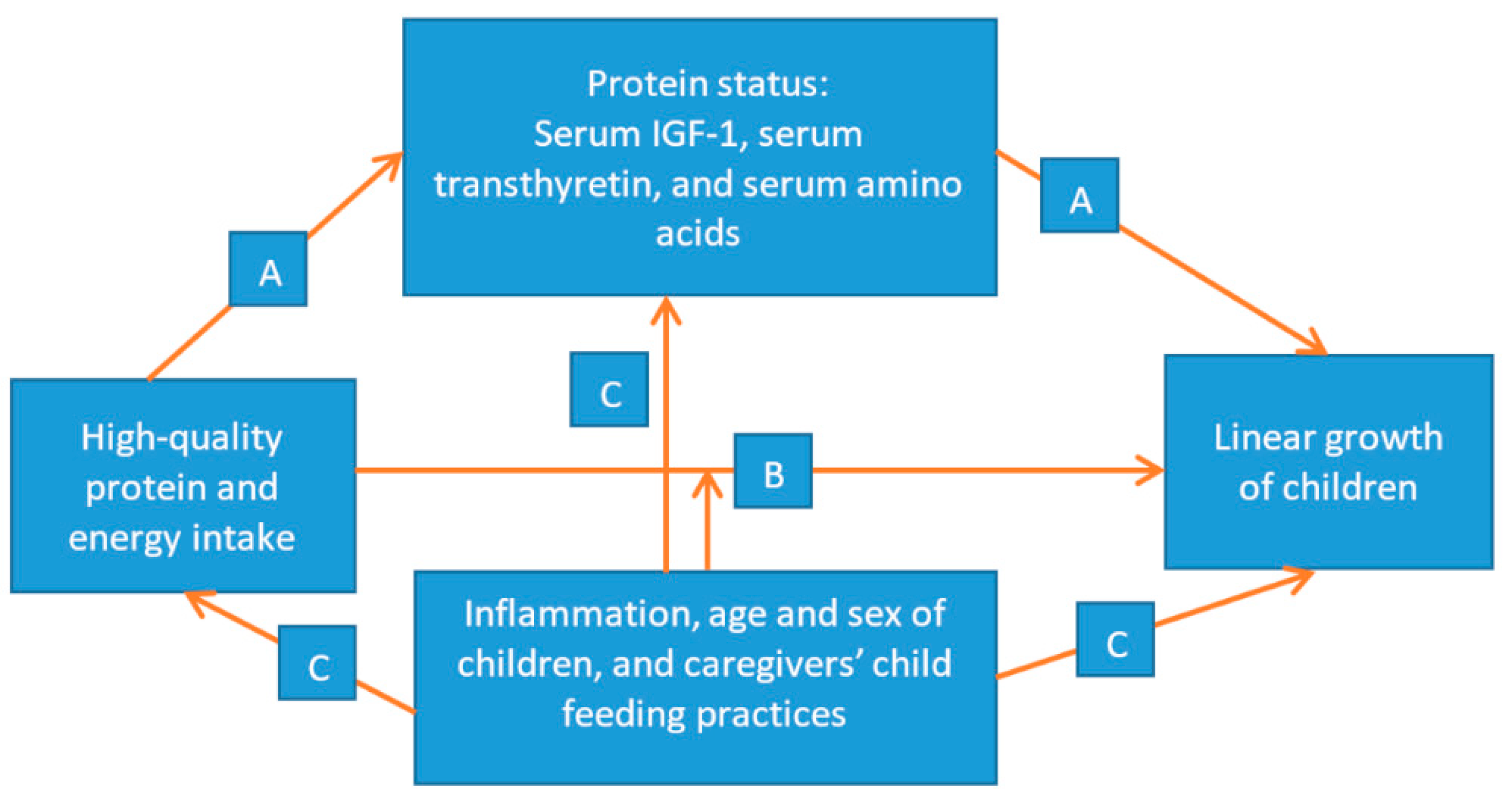
3.6. Association among High-Quality Protein Intake, Energy Intake, Serum Transthyretin, Serum Amino Acids, and Serum IGF-1 with the Linear Growth (Height-for-Age, HAZ) of Children
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Unicef, W.; World Bank Group. Unicef/Who/World Bank Group Joint Child Malnutrition Estimates 2018. Levels and Trends in Child Malnutrition. Key Findings of the 2018 Edition. 2018. Available online: http://www.who.int/nutgrowthdb/estimates/en (accessed on 15 August 2018).
- Development Initiatives. Global Nutrition Report 2017: Nourishing the Sdgs; Development Initiatives: Bristol, UK, 2017; Available online: http://globalnutritionreport.org/the-data/global-nutrition-profile (accessed on 21 May 2018).
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; De Onis, M.; Ezzati, M.; Grantham-Mcgregor, S.; Katz, J.; Martorell, R.; et al. Maternal, Child Nutrition Study G. Maternal and Child Undernutrition and Overweight in Low-Income and Middle-Income Countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Victora, C.G.; Adair, L.; Fall, C.; Hallal, P.C.; Martorell, R.; Richter, L.; Sachdev, H.S. Maternal, Child Undernutrition Study G. Maternal and Child Undernutrition: Consequences for Adult Health and Human Capital. Lancet 2008, 371, 340–357. [Google Scholar] [CrossRef]
- Devakumar, D.; Fall, C.H.; Sachdev, H.S.; Margetts, B.M.; Osmond, C.; Wells, J.C.; Costello, A.; Osrin, D. Maternal Antenatal Multiple Micronutrient Supplementation for Long-Term Health Benefits in Children: A Systematic Review and Meta-Analysis. BMC Med. 2016, 14, 90. [Google Scholar] [CrossRef] [PubMed]
- Semba, R. The Rise and Fall of Protein Malnutrition in Global Health. Ann. Nutr. Metab. 2016, 69, 79–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arsenault, J.E.; Brown, K. Effects of Protein or Amino-Acid Supplementation on the Physical Growth of Young Children in Low-Income Countries. Nutr. Rev. 2017, 75, 699–717. [Google Scholar] [CrossRef] [PubMed]
- Central Statistical Agency/CSA/ICF. Ethiopia Demographic and Health Survey 2016; CSA: Addis Ababa, Ethiopia; ICF: Rockville, MD, USA, 2016. [Google Scholar]
- Uauy, R.; Kurpad, A.; Tano-Debrah, K.; Otoo, G.E.; Aaron, G.A.; Toride, Y.; Ghosh, S. Role of Protein and Amino Acids in Infant and Young Child Nutrition: Protein and Amino Acid Needs and Relationship with Child Growth. J. Nutr. Sci. Vitaminol. 2015, 61, 192–194. [Google Scholar] [CrossRef] [PubMed]
- Hoffer, L. Human Protein and Amino Acid Requirements. Jpn. J. Parenter. Enter. Nutr. 2016, 40, 460–474. [Google Scholar] [CrossRef] [PubMed]
- Semba, R.D.; Trehan, I.; Gonzalez-Freire, M.; Kraemer, K.; Moaddel, R.; Ordiz, M.I.; Ferrucci, L.; Manary, M. Perspective: The Potential Role of Essential Amino Acids and the Mechanistic Target of Rapamycin Complex 1 (Mtorc1) Pathway in The Pathogenesis of Child Stunting. Adv. Nutr. 2016, 7, 853–865. [Google Scholar] [CrossRef] [PubMed]
- Millward, D. Nutrition, Infection and Stunting: The Roles of Deficiencies of Individual Nutrients and Foods, and of Inflammation, as Determinants of Reduced Linear Growth of Children. Nutr. Res. Rev. 2017, 30, 50–72. [Google Scholar] [CrossRef] [PubMed]
- Schonfeldt, H.C.; Gibson Hall, N. Dietary Protein Quality and Malnutrition in Africa. Br. J. Nutr. 2012, 108, S69–S76. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Fanzo, J.; Miller, D.D.; Pingali, P.; Post, M.; Steiner, J.L.; Thalacker-Mercer, A. Production and Supply of High-Quality Food Protein for Human Consumption: Sustainability, Challenges, and Innovations. Ann. N. Y. Acad. Sci. 2014, 1321, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Protein and Amino Acid Requirements in Human Nutrition. Report of A Joint WHO/FAO/UNU Expert Consultation. World Health Organization Technical Report Series 2007; Back Cover; pp. 1–265. Available online: Https://Www.Ncbi.Nlm.Nih.Gov/Pubmed/18330140 (accessed on 17 August 2017).
- Nuss, E.T.; Tanumihardjo, S. Quality Protein Maize for Africa: Closing the Protein Inadequacy Gap in Vulnerable Populations. Adv. Nutr. 2011, 2, 217–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hafebo, A.S.; Wuehler, S.; Gibbs, M.; Moges, T.; Tesfaye, B.; Kebede, A.; Assefa, T.; Zerfu, D.; Wedajo, B.; Abera, A. Overview of The Ethiopian National Food Consumption Survey (Nfcs): Implications for fortification Programs. Eur. J. Nutr. Food Saf. 2015, 5, 961–962. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Suri, D.; Uauy, R. Assessment of Protein Adequacy in Developing Countries: Quality Matters. Br. J. Nutr. 2012, 108, S77–S87. [Google Scholar] [CrossRef] [PubMed]
- Leistra, E.; Willeboordse, F.; Visser, M.; Weijs, P.J.; Haans-Van Den Oord, A.; Oostenbrink, J.; Evers, A.M.; Kruizenga, H. Predictors for Achieving Protein and Energy Requirements in Undernourished Hospital Patients. Clin. Nutr. 2011, 30, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Hoffer, L. Protein and Energy Provision in Critical Illness. Am. J. Clin. Nutr. 2003, 78, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Manary, M.; Callaghan, M.; Singh, L.; Briend, A. Protein Quality and Growth in Malnourished Children. Food Nutr. Bull. 2016, 37, S29–S36. [Google Scholar] [CrossRef] [PubMed]
- Kishi, K.; Miyatani, S.; Inoue, G. Requirement and Utilization of Egg Protein by Japanese Young Men with Marginal Intakes of Energy. J. Nutr. 1978, 108, 658–669. [Google Scholar] [CrossRef] [PubMed]
- Uauy, R. Keynote: Rethinking Protein. Food Nutr. Bull. 2013, 34, 228–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semba, R.D.; Shardell, M.; Sakr Ashour, F.A.; Moaddel, R.; Trehan, I.; Maleta, K.M.; Ordiz, M.I.; Kraemer, K.; Khadeer, M.A.; Ferrucci, L.; et al. Child Stunting is Associated with Low Circulating Essential Amino Acids. Ebiomedicine 2016, 6, 246–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, R. Principles of Nutritional Assessment; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- O’neill, B.T.; Lauritzen, H.P.; Hirshman, M.F.; Smyth, G.; Goodyear, L.J.; Kahn, C. Differential Role of Insulin/Igf-1 Receptor Signaling in Muscle Growth and Glucose Homeostasis. Cell Rep. 2015, 11, 1220–1235. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z. Insulin-Like Growth Factor 1 (Igf-1): A Growth Hormone. Mol. Pathol. 2001, 54, 311. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G.; Brown, K. Update on Technical Issues Concerning Complementary Feeding of Young Children in Developing Countries and Implications for Intervention Programs. Food Nutr. Bull. 2003, 24, 5–28. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G.; Adu-Afarwuah, S. Systematic Review of The Efficacy and Effectiveness of Complementary Feeding Interventions in Developing Countries. Matern. Child Nutr. 2008, 4, 24–85. [Google Scholar] [CrossRef] [PubMed]
- Tessema, M.; Gunaratna, N.S.; Donato, K.; Cohen, J.L.; Mcconnell, M.; Belayneh, D.; Brouwer, I.D.; Belachew, T.; De Groote, H. Translating the Impact of Quality Protein Maize into Improved Nutritional Status for Ethiopian Children: Study Protocol for A Randomized Controlled Trial. BMC Nutr. 2016, 2, 54. [Google Scholar] [CrossRef]
- Gibson, R.S.; Ferguson, E. An Interactive 24-H Recall for Assessing the Adequacy of Iron and Zinc Intakes in Developing Countries; International Food Policy Research Institute (IFPRI)/International Center for Tropical Agriculture (CIAT): Washington, DC, USA, 2008. [Google Scholar]
- Gewa, C.A.; Murphy, S.P.; Neumann, C. Out-of-Home Food Intake is often Omitted from Mothers’ Recalls of School Children’s Intake in Rural Kenya. J. Nutr. 2007, 137, 2154–2159. [Google Scholar] [CrossRef] [PubMed]
- Gewa, C.A.; Murphy, S.P.; Neumann, C. A Comparison of Weighed and Recalled Intakes for Schoolchildren and Mothers in Rural Kenya. Public Health Nutr. 2009, 12, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- EHNRI. Food Composition Table for Use in Ethiopia Part III; Ehnri: Addis Ababa, Ethiopia, 1997. [Google Scholar]
- EHNRI. Food Composition Table for Use in Ethiopia Part IV; Ehnri: Addis Ababa, Ethiopia, 1998. [Google Scholar]
- FAO. Available online: http://www.Fao.Org/Infoods/Infoods/En/ (accessed on 7 March 2017).
- Claro, R.M.; Levy, R.B.; Bandoni, D.H.; Mondini, L. Per Capita Versus Adult-Equivalent Estimates of Calorie Availability in Household Budget Surveys. Cadernos De Saúde Pública 2010, 26, 2188–2195. [Google Scholar] [CrossRef] [PubMed]
- Spackman, D.H.; Stein, W.H.; Moore, S. Automatic Recording Apparatus for Use in Chromatography of Amino Acids. Anal. Chem. 1958, 30, 1190–1206. [Google Scholar] [CrossRef]
- USP. Available online: Http://Www.Usp.Org/Harmonization-Standards/Pdg/Biotechnology/Amino-Acid-Determination (accessed on 5 October 2017).
- Union, E. Commission Regulation (Ec) Establishing Community Methods of Sampling and Analysis of Feedingstuffs. Off. J. Eur. Union 2009, 152, 23–32. [Google Scholar]
- Williams, J. Basic Laboratory Methods in Medical Parasitology; World Health Organization: Geneva, Switzerland, 1991. [Google Scholar]
- Ritchie, L. An Ether Sedimentation Technique for Routine Stool Examinations. Bull. U.S. Army Med. Dep. 1948, 8, 4. [Google Scholar]
- Child Growth Standards 2006; World Health Organization: Geneva, Switzerland, 2008.
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids. J. Am. Diet. Assoc. 2002, 102, 1621–1630. [Google Scholar] [CrossRef]
- What Global Nutrition Targets 2025: Stunting Policy Brief; World Health Organization: Geneva, Switzerland, 2012.
- Giugliani, E.R.; Victora, C. Complementary Feeding. J. Pediatr. 2000, 76, S253–S262. [Google Scholar] [CrossRef]
- Butte, N. Energy Requirements of Infants. Public Health Nutr. 2005, 8, 953–967. [Google Scholar] [CrossRef] [PubMed]
- Smith, W.J.; Underwood, L.E.; Clemmons, D. Effects of Caloric or Protein Restriction on Insulin-Like Growth Factor-I (Igf-I) and Igf-Binding Proteins in Children and Adults. J. Clin. Endocrinol. Metab. 1995, 80, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Gopalan, C.; Swaminathan, M.; Vijayaraghavan, K. Effect of Calorie Supplementation on Growth of Undernourished Childre. Am. J. Clin. Nutr. 1973, 26, 563–566. [Google Scholar] [CrossRef] [PubMed]
- Munro, H. Energy and Protein Intakes as Determinants of Nitrogen Balance. Kidney Int. 1978, 14, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.H.; Sanchez-Grinan, M.; Perez, F.; Peerson, J.M.; Ganoza, L.; Stern, J. Effects of Dietary Energy Density and Feeding Frequency on Total Daily Energy Intakes of Recovering Malnourished Children. Am. J. Clin. Nutr. 1995, 62, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Kurpad, A.V.; Regan, M.M.; Nazareth, D.; Nagaraj, S.; Gnanou, J.; Young, V. Intestinal Parasites Increase the Dietary Lysine Requirement In Chronically Undernourished Indian Men. Am. J. Clin. Nutr. 2003, 78, 1145–1151. [Google Scholar] [CrossRef] [PubMed]
- Pillai, R.R.; Elango, R.; Ball, R.O.; Kurpad, A.V.; Pencharz, P. Lysine Requirements of Moderately Undernourished School-Aged Indian Children Are Reduced by Treatment for Intestinal Parasites as Measured by the Indicator Amino Acid Oxidation Technique, 2. J. Nutr. 2015, 145, 954–959. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S. Protein Quality in the First Thousand Days of Life. Food Nutr. Bull. 2016, 37, S14–S21. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, D.G.; Martorell, R.; Rivera, J.A.; Ruel, M.T.; Habicht, J.-P. Age Differences in The Impact of Nutritional Supplementation on Growth. J. Nutr. 1995, 125, 1051s–1059s. [Google Scholar] [PubMed]
- Zhao, W.; Zhai, F.; Zhang, D.; An, Y.; Liu, Y.; He, Y.; Ge, K.; Scrimshaw, N. Lysine-fortified Wheat Flour Improves the Nutritional and Immunological Status of Wheat-Eating Families in Northern China. Food Nutr. Bull. 2004, 25, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Hussain, T.; Abbas, S.; Khan, M.A.; Scrimshaw, N. Lysine fortification of Wheat Flour Improves Selected Indices of The Nutritional Status of Predominantly Cereal-Eating Families in Pakistan. Food Nutr. Bull. 2004, 25, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Baron, J.; Sävendahl, L.; De Luca, F.; Dauber, A.; Phillip, M.; Wit, J.M.; Nilsson, O. Short and Tall Stature: A New Paradigm Emerges. Nat. Rev. Endocrinol. 2015, 11, 735. [Google Scholar] [CrossRef] [PubMed]
- Laplante, M.; Sabatini, D. Mtor Signaling in Growth Control and Disease. Cell 2012, 149, 274–293. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Palm, W.; Peng, M.; King, B.; Lindsten, T.; Li, M.O.; Koumenis, C.; Thompson, C. Gcn2 Sustains Mtorc1 Suppression Upon Amino Acid Deprivation by Inducing Sestrin2. Genes Dev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Gat-Yablonski, G.; De Luca, F. Effect of Nutrition on Statural Growth. Horm. Res. Paediatr. 2017, 88, 46–62. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, C.; Udam, T.R.; Lauritzen, L.; Mølgaard, C.; Juul, A.; Michaelsen, K. Animal Protein Intake, Serum Insulin-Like Growth Factor, I.; and Growth in Healthy 2.5-Y-Old Danish Children. Am. J. Clin. Nutr. 2004, 80, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Yakar, S.; Isaksson, O. Regulation of Skeletal Growth and Mineral Acquisition by the Gh/Igf-1 Axis: Lessons from Mouse Models. Growth Horm. IGF Res. 2016, 28, 26–42. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.L.; Stein, A. The Impact of Nutritional Interventions Beyond the First 2 Years of Life on Linear Growth: A Systematic Review and Meta-Analysis. Adv. Nutr. 2017, 8, 323–336. [Google Scholar] [CrossRef] [PubMed]
- Forrestal, S.G. Energy Intake Misreporting Among Children and Adolescents: A Literature Review. Matern. Child Nutr. 2011, 7, 112–127. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Indicators | All Households (n = 868) | Households with Stunted Child (n = 258) | Households with Non-Stunted Child (n = 610) |
|---|---|---|---|
| Caregiver age (years), Median (Q1, Q3) | 28 (25, 32) | 28 (25, 32) | 28 (25, 32) |
| Caregiver relationship to the household head, % | |||
| Household head | 3 | 2 | 4 |
| Spouse | 96 | 97 | 96 |
| Other | 1 | 1 | - |
| Caregiver with no formal education, % | 65 | 67 | 64 |
| Religion, % | |||
| Christian | 62 | 61 | 63 |
| Muslim | 38 | 39 | 37 |
| Family size, Median [Q1, Q3] | 6 [5, 8] | 6 [5, 7] | 6 [5, 8] |
| Wealth tertiles 1, % | |||
| 1st tertile (poorer) | 33 | 37 | 31 * |
| 2nd tertile | 33 | 37 | 32 * |
| 3rd tertile (wealthier) | 33 | 26 | 37 * |
| Variables | Total (n = 868) | Stunted (n = 258) | Non-Stunted (n = 610) |
|---|---|---|---|
| Female, %, | 48 | 44 | 49 |
| Age in months, Median (Q1, Q3) | 20 (13, 27) | 23 (16, 28) | 19 (12, 26) |
| Vitamin A supplementation in the last six months, % | 83 | 84 | 83 |
| Any multivitamin in the last six months, % | 4 | 6 | 4 |
| Iron tablets/syrups in the last six months, % | 1 | 2 | 1 |
| Any drugs for intestinal worms in the last six months, % | 22 | 24 | 21 |
| Diarrhea in the two weeks before survey, % | 18 | 17 | 18 |
| Cough or breathing problems in the two weeks before the survey, % | 17 | 15 | 18 |
| Fever in the two weeks before the survey, % | 19 | 20 | 19 |
| HAZ (overall), Mean ± SD | −1.3 ± 1.3 | −2.8 ± 0.7 | −0.7 ± 1.0 |
| Variables | Total (n = 868) | Stunted (n = 258) | Non-Stunted (n = 610) |
|---|---|---|---|
| Protein intake (g/day) 2 | 16 (12, 22) | 16 (11, 21) | 16 (12, 22) |
| Lysine intake (mg/day) 2 | 589 (349, 859) | 541 (333, 813) | 597 (356, 868) |
| Tryptophan intake (mg/day) 2 | 233 (164, 343) | 205 (142, 284) | 246 (173, 369) * |
| Proportion of children with low protein intake (below EAR), % 3 | 10.5 | 10 | 11 |
| Proportion of children with low lysine intake (below EAR), % 3 | 31 | 30 | 31 |
| Proportion of children with low tryptophan intake (below EAR), % 3 | 4 | 4 | 4 |
| Variables | Total (n = 868) | Stunted (n = 258) | Non-Stunted (n = 610) |
|---|---|---|---|
| Energy intake (kcal/day) 2 | 695 (519, 870) | 643 (463, 818) | 703 (550, 891) * |
| Proportion of children with low energy intake (below EAR), % 3 | 76 | 85 | 72 * |
| Energy density (kcal/g) 2 | 1.4 (1.2, 1.6) | 1.4 (1.2, 1.6) | 1.3 (1.2, 1.6) |
| Variables 1 | Total (n = 868) | Stunted (n = 258) | Non-Stunted (n = 610) |
|---|---|---|---|
| Serum transthyretin (g/L) | 0.17 (0.14, 0.20) | 0.17 (0.14, 0.19) | 0.17 (0.14, 0.21) |
| Serum IGF-1 (ng/mL) | 30 (22, 44) | 26 (19, 36) | 32 (23, 46) * |
| Serum lysine (µmol/L) | 141 (116, 164) | 138 (116, 159) | 142 (117, 167) |
| Serum tryptophan (µmol/L) | 42 (32, 51) | 39 (23, 49) | 42 (34, 51) * |
| AGP (g/L) | 0.84 (0.65, 1.12) | 0.83 (0.65, 1.11) | 0.85 (0.65, 1.12) |
| CRP (mg/L) | 0.67 (0.32, 2.03) | 0.75 (0.32, 1.77) | 0.65 (0.31, 2.11) |
| Prevalence of inflammation (acute and/or chronic), % 2 | 35 | 35 | 35 |
| Prevalence of one or more intestinal parasites, % | 48 | 50 | 46 |
| Indicators | HAZ | WHZ | Serum Transthyretin (g/L) | Serum Lysine (µmol/L) | Serum Tryptophan (µmol/L) | Serum IGF-1 (ng/mL) | AGP (g/L) | CRP (mg/L) | Lysine Intake (mg/kg/Day) | Tryptophan Intake (mg/kg/Day) | Protein Intake (g/Day) | Energy Intake (kcal/Day) | Intestinal Parasites |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WHZ | 0.11 ** | ||||||||||||
| Serum transthyretin (g/L) | 0.08 | 0.12 ** | |||||||||||
| Serum lysine (µmol/L) | 0.06 | 0.04 | 0.13 * | ||||||||||
| Serum tryptophan (µmol/L) | 0.18 ** | 0.01 | 0.25 *** | 0.55 *** | |||||||||
| Serum IGF-1 (ng/mL) | 0.12 ** | 0.16 ** | 0.22 *** | 0.02 | 0.07 | ||||||||
| AGP (g/L) | −0.02 | −0.02 | −0.37 *** | −0.11 * | −0.23 *** | −0.1 *** | |||||||
| CRP (mg/L) | 0.005 | −0.05 | −0.32 *** | −0.13 * | −0.11 *** | −0.08 * | 0.51 *** | ||||||
| Lysine intake (mg/kg/day) | −0.01 | −0.1 * | −0.03 | 0.01 | −0.08 | −0.09 | 0.01 | 0.09 | |||||
| Tryptophan intake (mg/kg/day) | 0.12 ** | −0.069 | −0.055 | 0.071 | 0.074 | −0.042 | −0.002 | 0.019 | 0.68 *** | ||||
| Protein intake (g/day) | 0.10 * | 0.06 | −0.01 | 0.04 | −0.05 | −0.07 | 0.03 | 0.04 | 0.74 ** | 0.47 ** | |||
| Energy intake (kcal/day) | 0.13 ** | 0.07 | −0.02 | 0.01 | −0.03 | −0.08 | 0.01 | 0 | 0.68 ** | 0.55 ** | 0.88 *** | ||
| Intestinal parasites | −0.05 | −0.1 *** | −0.05 | 0.05 | −0.01 | 0.01 | 0.03 | 0.04 | 0.01 | 0.03 | −0.03 | −0.01 | |
| Wealth index | 0.1 ** | 0.11 ** | 0.01 | 0.04 | 0.01 | 0.04 | 0.004 | 0.05 | 0.09 * | 0.03 | 0.01 | 0.01 | 0.01 |
| (A) | ||||||||||||||||||
| Models | Model 1 | Model 2 | Model 3 | Model 4 | ||||||||||||||
| Fixed Effects | b | SE | p | b | SE | p | b | SE | p | b | SE | p | ||||||
| Intercept | −1.04 | 0.24 | <0.0001 | −1.10 | 0.26 | <0.0001 | −1.07 | 0.33 | 0.001 | −0.89 | 0.24 | 0.0002 | ||||||
| Protein intake (g/day) | 0.01 | 0.005 | 0.01 | |||||||||||||||
| Energy intake (kcal/day) | 0.0003 | 0.0002 | 0.04 | |||||||||||||||
| Serum transthyretin (g/L) | 2.58 | 1.24 | 0.04 | |||||||||||||||
| Serum IGF-1 (ng/mL) | 0.01 | 0.003 | 0.0004 | |||||||||||||||
| Serum AGP(g/L) | 0.11 | 0.18 | 0.54 | 0.11 | 0.18 | 0.53 | −0.06 | 0.16 | 0.70 | −0.12 | 0.16 | 0.44 | ||||||
| Serum CRP (mg/L) | −0.001 | 0.01 | 0.88 | −0.0005 | 0.01 | 0.92 | 0.01 | 0.005 | 0.25 | 0.004 | 0.005 | 0.37 | ||||||
| Intestinal parasites | −0.07 | 0.12 | 0.55 | −0.08 | 0.12 | 0.51 | −0.10 | 0.12 | 0.40 | −0.08 | 0.11 | 0.47 | ||||||
| (B) | ||||||||||||||||||
| Models | Model 1 | Model 2 | Model 3 * | Model 4 * | Model 5 * | Model 6 * | ||||||||||||
| Fixed effects | b | SE | p | b | SE | p | b | SE | p | b | SE | p | b | SE | p | b | SE | p |
| Intercept | −1.26 | 0.09 | <0.0001 | −1.549 | 0.0948 | <0.0001 | −0.70 | 0.24 | 0.004 | −0.63 | 0.29 | 0.03 | −0.40 | 0.39 | 0.31 | −0.92 | 0.39 | 0.02 |
| Lysine intake per kg body weight (mg/kg/day) | −0.0004 | 0.001 | 0.69 | −0.002 | 0.001 | 0.11 | ||||||||||||
| Tryptophan intake per kg body weight (mg/kg/day) | 0.01 | 0.003 | 0.001 | −0.004 | 0.003 | 0.23 | ||||||||||||
| Serum lysine (µmol/L) | −0.0003 | 0.002 | 0.89 | |||||||||||||||
| Serum tryptophan (µmol/L) | 0.01 | 0.005 | 0.10 | |||||||||||||||
| Serum AGP(g/L) | 0.10 | 0.18 | 0.58 | 0.10 | 0.18 | 0.58 | −0.32 | 0.19 | 0.09 | −0.25 | 0.19 | 0.20 | ||||||
| Serum CRP (mg/L) | 0.0002 | 0.01 | 0.96 | −0.00002 | 0.01 | 1.00 | 0.01 | 0.01 | 0.13 | 0.01 | 0.01 | 0.14 | ||||||
| Intestinal parasites | −0.08 | 0.12 | 0.52 | −0.07 | 0.12 | 0.57 | −0.01 | 0.14 | 0.96 | −0.01 | 0.14 | 0.95 | ||||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tessema, M.; Gunaratna, N.S.; Brouwer, I.D.; Donato, K.; Cohen, J.L.; McConnell, M.; Belachew, T.; Belayneh, D.; De Groote, H. Associations among High-Quality Protein and Energy Intake, Serum Transthyretin, Serum Amino Acids and Linear Growth of Children in Ethiopia. Nutrients 2018, 10, 1776. https://doi.org/10.3390/nu10111776
Tessema M, Gunaratna NS, Brouwer ID, Donato K, Cohen JL, McConnell M, Belachew T, Belayneh D, De Groote H. Associations among High-Quality Protein and Energy Intake, Serum Transthyretin, Serum Amino Acids and Linear Growth of Children in Ethiopia. Nutrients. 2018; 10(11):1776. https://doi.org/10.3390/nu10111776
Chicago/Turabian StyleTessema, Masresha, Nilupa S. Gunaratna, Inge D. Brouwer, Katherine Donato, Jessica L. Cohen, Margaret McConnell, Tefera Belachew, Demissie Belayneh, and Hugo De Groote. 2018. "Associations among High-Quality Protein and Energy Intake, Serum Transthyretin, Serum Amino Acids and Linear Growth of Children in Ethiopia" Nutrients 10, no. 11: 1776. https://doi.org/10.3390/nu10111776